Research Overview
About the MRC/Wits-Agincourt Unit
 The Agincourt Health and Socio-Demographic Surveillance System (HDSS), located in in rural northeast South Africa close to the Mozambique border, provides the foundation for the Rural Public Health and Health Transitions Research Unit of the Medical Research Council (MRC) and University of the Witwatersrand, South Africa (the MRC/Wits-Agincourt Unit). Its origins lie in the university’s ‘Health Systems Development Unit’ that in the early 1990s focused on district health systems development, sub-district health centre networks and referral systems and training of clinically oriented primary health care nurses. The Agincourt HDSS was a founding member of the International Network for the Demographic Evaluation of Populations and Their Health (INDEPTH) (www.indepth-network.org)
The Agincourt Health and Socio-Demographic Surveillance System (HDSS), located in in rural northeast South Africa close to the Mozambique border, provides the foundation for the Rural Public Health and Health Transitions Research Unit of the Medical Research Council (MRC) and University of the Witwatersrand, South Africa (the MRC/Wits-Agincourt Unit). Its origins lie in the university’s ‘Health Systems Development Unit’ that in the early 1990s focused on district health systems development, sub-district health centre networks and referral systems and training of clinically oriented primary health care nurses. The Agincourt HDSS was a founding member of the International Network for the Demographic Evaluation of Populations and Their Health (INDEPTH) (www.indepth-network.org)
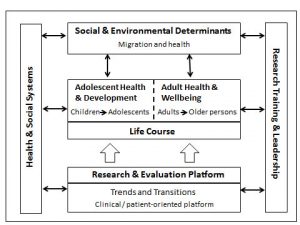
Framework highlighting key research areas of the MRC/Wits-Agincourt Unit
COVID-19 Response
Health & Social Systems

The dynamics of health transition are reflected in the burdens affecting rural adults. Studies are occurring in epidemiology and treatment of epilepsy as well as the health and wellbeing of ageing populations.Theme Leader:
Steve Tollman
Overview
Adolescent Health & Development

In rural South Africa morbidity, mortality and growth failure associated with malnutrition exist alongside female obesity and emerging cardiovascular disease. By tackling proximal issues of infant growth and nutrition, and social and emotional development in children, we aim to impact more distal outcomes including cognitive development, educational attainment, and adult metabolic disease.Theme Leaders:
Kathy Kahn and Shane Norris
Overview
Research & Evaluation Platform – Trends and Transitions

This theme seeks to understand dynamics of demographic and epidemiological change in rural populations undergoing rapid and multiple transitions, and to identify the forces driving that change.Theme Leader:
Mark Collinson
Overview
Adult Health & Wellbeing

The Agincourt Unit is examining the immediate and longer term impacts of HIV/AIDS and antiretroviral therapy roll-out. This work will support provincial and national efforts and provide evidence on delivery models, coverage and individual and population impacts of ARTs, as well as efforts to improve chronic disease treatment.Theme Leaders:
Steve Tollman
F. Xavier Gómez-Olivé
Overview
Social & Environmental Determinants

Rural households remain under pressure. Sudden shocks, whether job loss or death of a breadwinner, can destabilise households; similarly, protracted stresses such as drought or chronic illness can undermine coping capacity and livelihoods. Key to understanding how to improve health and social development is to examine the strategies employed by households to gain livelihoods and cope with shocks and stresses.Theme Leaders:
Mark Collinson
Overview
Features of cohorts nested within the MRC/Wits-Agincourt Unit, 2018
| |
Cohort description |
Sample |
| Cohort name |
Aim |
Size |
Type |
Assessments to-date
Frequency of follow-up |
Inclusion
criteria |
Sampling unit |
|
OBSERVATIONAL COHORTS
|
|
|
|
|
|
| INDEPTH-SAGE (Survey on global AGEing and adult health)
|
To assess health status, wellbeing and health seeking behaviour of older persons |
4509 |
Open |
Baseline in 2006
Follow-up in 2010
Repeated 2013
Repeat in 2018
|
Population 50 years and older
Permanent residents |
Individual |
| HAALSI
(Health & Ageing in Africa: Longitudinal Study of an INDEPTH community) |
Longitudinal follow-up of functional, physical and cognitive assessments, and biomarker measurement to identify biological, social, and economic predictors of mortality; incidence of disease and onset of new events; changes in physical and cognitive function.
|
5059 |
Open |
Baseline 2014-2015
Follow up 2018
Follow up 2021 |
Permanent residents in study site in 2013, both sexes, 40 years and older |
Individual |
| AWIGEN
(Africa Wits-INDEPTH genomic studies of cardiovascular disease) |
Expand genomic association studies; deepen understanding of genome architecture and population structure; strengthen genomic and bioinformatics research capacity; modify and develop tools to study African populations.
To develop community engagement strategies and approach to feedback results to communities.
|
2486
1465 (40-60 years)
1021 (>60 years) |
Open |
Baseline 2014-2015
Follow up 2018
Follow up 2021 |
Permanent residents in study site in 2013, both sexes, 40 – 60 years. Population >60 years integrated with HAALSI |
Individual |
| PHIRST
(Prospective Household study of Influenza, Respiratory Syncytial virus and other respiratory pathogens community burden and Transmission dynamics) |
To estimate the community burden of influenza and RSV, and to assess the transmission dynamics of influenza and RSV infections in the community |
200 households to get sample of 1500 individuals per year |
Open |
First selection 2016
Second selection 2017
Third selection 2018 |
Randomly selected households residing in the communities for at least 1 year prior to start of study and planning to stay; all members of household consent to participate; households should have with at least 3 individuals; 50% of households with at least 1 child aged <5 |
Household (all individuals in the HH are selected) |
|
MHFUS
(Migration & health follow-up study) |
To describe, at individual level, how a contemporary, complex pattern of migration and urbanization helps drive the health transition in low and middle income countries. To conduct a new observational study to understand how migrants acquire and manage chronic diseases and access long-term care
|
3000 |
Open |
Baseline 2017-2018
Rounds 2 & 3 in 2019 and 2020 by phone call
Round 4 in person 2020
Round 5 2021 by phone |
Residents in the study site in 2016, both sexes,18 – 49 years
|
Individual |
| CLINIC LINK |
Link HDSS members 18 years + with clinic records to measure chronic care utilization in the Primary Health Care system
|
All PHC clients |
Open |
Linkage started in 2014 |
Members of HDSS 18 years and older who attend any PHC service in the study site for HIV or chronic care
|
Individual |
| ABACUS
(Antibiotic access and use study) |
Primary aim: to compare sociocultural determinants of appropriate access and use of antibiotics between 6 different LMICs.
|
600 |
Open |
Baseline in 2018 and follow up 6 months after the first visit. |
Households of the HDSS who consent to participate. |
Household |
| ARK
(African Research into Kidney disease) |
Determine true prevalence of CKD in SA; develop and validate age- and gender-based prediction equation for estimating glomerular filtration rate in Africans; establish risk factors associated with CKD in South Africa
|
1800 |
Open |
Baseline 2017-2018
Follow up 2018-2019 |
Permanent residents in study site in 2016, both sexes, ≥ 18 years of age |
Individual |
| Ha Nakekela
(‘We care’) |
Measure HIV and non-communicable disease prevalence and their risk factors |
7428 |
Closed |
Baseline 2010/2011
Repeat planned in 2013 |
Men and women
15 years and older Permanent residents
|
Individual |
| SEEDS
(Study of the Epidemiology of Epilepsy) |
To understand the burden of epilepsy, pattern of seizures, and excess mortality in persons with epilepsy
|
310 |
Closed |
Nine rounds every 3 months completed in 2012 and 2013
Follow-up 2018
Tracking through HDSS
|
All ages diagnosed with epilepsy following screening in 2008 |
Individual |
| SUCSES (Sustainability in Communal Socio-Ecological Systems) |
To examine (i) household income, resource use, response to shocks, (ii) how livelihood capital, migration and use of natural resources shape household resilience and (iii) how poverty influences child nutrition |
590 |
Closed |
Round 1 – 2010
Round 2 – 2011
Round 3 – 2012
Follow up – 2019 |
Sample stratified by gender and age
Four individuals selected per age/gender group in nine villages |
Individual (households interviewed) |
Features of interventions and trial cohorts nested within the MRC/Wits-Agincourt Unit, 2017
|
|
Cohort description |
Sample |
|
|
Cohort name |
Aim |
Size |
Type |
Assessments to-date
Frequency of follow-up |
Inclusion
criteria |
Sampling unit |
|
|
|
|
|
|
|
|
|
|
| INTERVENTION / TRIAL COHORTS |
| Swa Koteka
(‘It is possible’
HPTN068
Conditional cash transfer trial) |
To determine whether young women randomized to receive CCTs conditional on school attendance have lower incidence of HIV infection over time compared to young women not randomized to receive cash transfers |
2537 |
Open |
Baseline 2011
First round 2012
Second round 2013
Third round 2014
Follow up 2015
Follow up 2017
Follow up 2018/19
|
Female; age 13-20; enrolled in grades 8-11; not married or pregnant; able to read; able to open bank accountt; parent/ guardian able to open bank account; residing in study area and intending to remain
|
Individual |
| Nkateko
(‘Blessing’) |
To reduce population levels of uncontrolled hypertension, especially in those individuals at greatest risk, by supporting and strengthening the management of hypertension in primary care clinics |
3770 in 2013
3015 in 2015 |
Closed |
Two cross sectional studies 2013 and 2015
Participants linked to clinics records |
Adults over 18 years and residing in Agincourt sub-district.
All adults attending a clinic. |
Individual for cross-sectional.
Clinics as clusters for trial |
| Nhluvuko
(‘Development’ -HIV self-testing) |
To determine impact of HIV self-testing compared to HCT on testing uptake and frequency, referral and usage among peers/ partners, return for confirmatory testing and linking to care. To assess need for follow-up and linkage to care, as well as support materials for optimal and safe use of self-testing
|
400 |
Open |
Baseline 2017
Follow up after 3 and 6 months
Linked to HDSS |
Young women 18-26 years from study site |
Individual |
| One Man Can |
Cluster randomised trial to assess impact of community mobilization intervention on gender norms
|
2400 |
Open |
Baseline 2012
Endline 2015 |
Young men 18-35 years |
Cluster |
| Tsima
(‘Help each other’)
|
To evaluate theory-driven community-level interventions to improve uptake of testing, linkage to and retention in care for HIV positive individuals in high prevalence setting |
7 control and 8 intervention villages |
Open |
Cross-sectional in 2015
Cross-sectional in 2018
Clinical records of all clinic attendees linked to HDSS |
Lived in the study area for 12 months, 18-49 years, 1 individual per household |
Village clusters
Individual for cross-sectional studies |