Theme leaders: Steve Tollman and F. Xavier Gómez-Olivé

Photo by Lisa Alberts
CURRENT PROJECTS
Timing, quality, and physiology of sleep in a deprived community cohort in South Africa and their relationship with chronic disease
PIs: Prof Xavier Gómez-Olivé (University of the Witwatersrand, South Africa) and Prof. Malcolm von Schantz (University of Surrey, UK)
Collaborators: Dr Alison Bentley, Dr Karine Scheuermeier and Dr. Johanna Roche (University of the Witwatersrand, South Africa); Dr Kristen Knutson (Northwestern University, USA); Dr Francieli Ruiz da Silva and Katie O’Brien (University of Surrey, UK); Dr. Laura Roden (Coventry University, UK); and Dr Dale Rae (University of the Cape Town, South Africa).
Maintaining a good and healthy sleep pattern is a potential low-cost intervention to prevent disease, which is not always easy in unequal societies in rural Africa where people may have to sleep under uncomfortable and unsafe conditions. There is a general shortage of data on sleep patterns in rural Africa and the effect of HIV infection and anti-retroviral medication on sleep and mental physical health. Our work is aiming to describe the sleep patterns in rural South Africa and to understand the association between sleep patterns and chronic conditions, like hypertension and diabetes, as well as the relationship between sleep and HIV infection. Therefore, this study aims to fill a research gap that has particular relevance to Africa, and worldwide significance.
In this study we are aiming to recruit participants from the existing HAALSI cohort in Agincourt using the Pittsburg Sleep Quality Index, Insomnia Severity Index and Munich Chronotype Questionnaire. To date, we have collected questionnaire data; physical activity, sleep habits and light exposure for 7 days using a wrist-worn activity monitor; polysomnography (PSG), full sleep recordings including brain activity, breathing, ECG, and oxygen levels; and melatonin levels using the Dim Light Melatonin Onset (DLMO) test. These are the first full PSG home recordings collected in rural Africa, providing important proof of concept for the feasibility of the method as well as datasets relevant to the living conditions of Africans. The main finding of our study so far is an alarming prevalence of obstructive sleep apnoea (OSA) in 29% of the participants studied to date.
For more information on this project please email Professor Francesc Xavier Gómez-Olivé at f.gomez-olivecasas@wits.ac.za.
AWI-Gen (Africa, Wits-INDEPTH Partnership for the GENomic study of body composition and CMD risk) Feb 2017
Michele Ramsay, Osman Sankoh, Steve Tollman and colleagues
AWI-Gen is a Collaborative Centre that is part of the Human Heredity and Health in Africa (H3Africa) Consortium (www.H3Africa.org). The long-term vision of AWI-Gen is to build sustainable capacity for research that leads to an understanding of the interplay between genetic, epigenetic and environmental risk factors for obesity and related cardiometabolic diseases (CMD) in sub-Saharan Africa. Under the auspices of the University of the Witwatersrand (Wits) and the International Network for the Demographic Evaluation of Populations and Their Health in Low- and Middle- Income Countries (INDEPTH), it will capitalize on the unique strengths of existing longitudinal cohorts, including the urban Soweto and rural Agincourt studies in South Africa (Wits based), and the well established INDEPTH health and demographic surveillance centres (HDSS) in Kenya, Ghana, Burkina Faso and South Africa. The centers offer established infrastructure, trained fieldworkers, long-standing community engagement, and detailed longitudinal phenotypic data, focusing on obesity and cardiometabolic health. Key strengths are harmonized phenotyping across sites, building on strong existing cohorts, and representation of the geographic and social variability of African populations. We aim to: 1. Build sustainable infrastructure (biobanks and laboratories) and capabilities (well characterized population cohorts, genotyping and bioinformatics) for genomic research on the African continent; 2. Understand the genomic architecture of sub-Saharan populations from west, east and south Africa to guide genomic studies (high throughput SNP and CNV arrays using unrelated individuals and family trios to improve the accuracy of haplotype analyses) and; 3. Investigate the independent and synergistic genomic contributions to body fat distribution (BMI, hip/waist circumference, subcutaneous and visceral fat) in these populations considering the relevant environmental and social contexts (rural/urban communities, quickly transitioning obesity prevalence, differential HIV, TB, and malaria infection histories). We will investigate the effect of obesity and fat distribution on the risk for CMD in the longitudinal cohorts. Recruitment of just over 12,000 participants was completed at the end August 2016 and data analysis is in progress. The second round of data collection will start in September 2019.
OUTPUTS
Engelbert A. Nonterah, Palwende R. Boua, Kerstin Klipstein‐Grobusch, Gershim Asiki, Lisa K. Micklesfield et al. Classical Cardiovascular Risk Factors and HIV are Associated with Carotid Intima‐Media Thickness in Adults From Sub‐Saharan Africa: Findings From H3Africa AWI‐Gen Study: 3 Jul 2019https://doi.org/10.1161/JAHA.118.011506
AWI-Gen Pilot Microbiome Project: Gut microbiome profile and cardiometabolic health Feb 2018
Collaboration with the Sydney Brenner Institute for Molecular Bioscience and Ami Bhatt, Stanford and Matt McQueen, University of Colorado, Boulder
Recent research has shown that gut microbiome is a very powerful biomarker of cardio-metabolic health, with a complex relationship between diet, lifestyle, microbiome and health. Dysbiosis in the gut microbiome is associated with a number of adverse cardiometabolic conditions. A health bacterial eco-system is thought to be very important in nutrition, helping repel pathogens and regulating the immune system. There has been little research in African environments, and this study will be an important initial study in this region.

Scott Hazelhurst (SBIMB), Ami Bhatt & Fiona Tamburini (Stanford) with MRC/Wits-Agincourt Community Advisory Group members
In this pilot study we have collected fecal samples from 96 women in the MRC/Wits-Agincourt study area. As they were part of the HAALSI study, we have extensive information about them. DNA will be extracted from the sample, and the bacterial population will be profiled using analyses of the 16S RNA gene. This will enable to us to determine the range of bacterial communities in individuals and whether and how different profiles are associated with different cardiometabolic outcomes. A subset of the samples will have shotgun or deep sequencing done which will help us not only determine what bacteria is there, but what their function is. A companion study is being carried out in Soweto by the DPHRU. If successful, more extensive studies will be carried out as part of the next round of the AWI-Gen and HAALSI projects. In January 2019, the team presented data and ideas for future studies to the Community Advisory Board, clinic sisters and villages leaders in the Agincourt study area. Here is a fact sheet that was developed for this workshop.
HAALSI – Health and Aging in Africa: Longitudinal Studies of an INDEPTH community Feb 2019
PIs: Lisa Berkman and Stephen Tollman.
Collaborating institutions – Centre for Population and Development Studies, Harvard School of Public Health, Harvard University, USA; INDEPTH Network, Ghana; Center for Health Policy and Center for Primary Care Outcomes and Research, Stanford University, USA; Heidelberg Institute for Global Health, University of Heidelberg, Germany; Centre for Global Health Research, Umeå University, Sweden.

HAALSi – An eco-social framework
This study is designed to longitudinally examine the biological, social, and economic conditions that shape health in the aging population. The MRC/Wits-Agincourt Unit HAALSI cohort was established with baseline data for 5,059 men and women ≥40 years of age. The study was renewed for 5 years with funding from the National Institute of Aging. During 2017-2021, two waves of follow-up data collection will be conducted to facilitate a longitudinal analysis of morbidity; mortality; biological, behavioral, and environmental risk factors; and physical and cognitive function.
HAALSi – Integration of projects
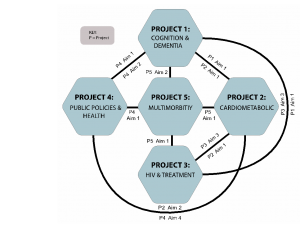
The HAALSI Program includes five projects: Project 1: Dementia and Cognitive Impairment; Project 2: Cardiometabolic Disease in an Aging South African Cohort; Project 3: HIV and HIV Interventions to Promote Healthy Aging; Project 4: Public Policies to Improve Healthy Aging; and Project 5: Multimorbidity. The projects will be supported by four cores: Leadership and Administration (Core A), Field (Core B), Data Management and Analysis (Core C), Biomarkers and Biobanking (Core D). Our study sets out to identify and examine the distribution of both novel and established risk factors for chronic health conditions and conduct follow-up to discover the predictive value of the biological, social, and environmental risk factors. The HAALSI Program study design is finely tuned to capture characteristics specific to South Africa as well as harmonize and conduct cross country comparative research with other HRS sister studies in India, China, Mexico, the UK, Europe, and the United States, providing a unique opportunity to conduct cross-country comparisons of the biological, social, and economic determinants of chronic diseases and their effects on functional and health outcomes in ageing populations.
Feedback about this study was given to all of the communities in the Agincourt HDSS in the form of an informative, one-page fact sheet. To see the fact sheet, click here.
OUTPUTS
- . 2019. “Multimorbidity and care for hypertension, diabetes and HIV among older adults in rural South Africa.” Bulletin of the World Health Organization, 97, 1, Pp. 10-23.
- . 2019. “Cognitive Function and Impairment in Older, Rural South African Adults: Evidence from “Health and Aging in Africa: A Longitudinal Study of an INDEPTH Community in Rural South Africa”.” Neuroepidemiology, 52, 1-2, Pp. 32-40
- . 2019. “Hypertension and diabetes control along the HIV care cascade in rural South Africa.” Journal of the International AIDS Society, 22, 3, Pp. e25213
- . 2019. “High Sedentary Behavior Is Associated with Depression among Rural South Africans.” International Journal of Environmental Research and Public Health, 16, 8.
- . 2019. “Chronic multimorbidity among older adults in rural South Africa.” BMJ Global Health, 4, 4.
- Article in The Conversation about how unhealthy ageing takes its toll on health and income
- First official fact sheet of the year 2018
- Jennifer Manne-Goehler, Julia Rohr, Livia Montana, Mark Siedner, Guy Harling, F. Xavier Gómez-Olivé, Pascal Geldsetzer, Ryan Wagner, Lubbe Wesner, Kathleen Kahn, Stephen Tollman, Till W. Bärnighausen. ART denial: results of a home-based study to validate self-reported antiretroviral use in rural South Africa. AIDS Behav. 2019 August ; 23(8): 2072–2078. doi:10.1007/s10461-018-2351-7
- Link to the HAALSi website here.
- Guy Harling, Collin F. Payne, Justine I. Davies, F. Xavier Gomez-Olive, Kathleen Kahn, Lenore Manderson, Farrah J. Mateen, Stephen M. Tollman, Miles D. Witham, BMBCh, PhD. Impairment in Activities of Daily Living, Care Receipt, and Unmet Needs in a Middle-Aged and Older Rural South African Population: Findings From the HAALSI Study. Journal of Aging and Health
1-27. 2019. - Harling, G., Payne, C. F., Davies, J. I., Gomez-Olive, F. X., Kahn, K., Manderson, L., … Witham, M. D. (2019). Impairment in Activities of Daily Living, Care Receipt, and Unmet Needs in a Middle-Aged and Older Rural South African Population: Findings From the HAALSI Study. Journal of Aging and Health. https://doi.org/10.1177/0898264318821220
HIV/Diabetes (sub- study of HAALSi) Feb 2019
In South Africa, the prevalence of Type 2 diabetes is estimated at 9.0% among those aged 30 and above. The International Diabetes Federation has projected that the prevalence of diabetes will double by 2030 in sub-Saharan Africa. Though the causes of the projected increase have not been fully characterized, some research suggests diet change, decreases in physical activity and urbanization may all play a role. Furthermore, the HIV epidemic may be a potential driver of this increase in part because ART medications including many first-line drugs used in South Africa are known to increase risk of metabolic syndrome, though more research is needed. There are two aims of the HIV-Diabetes study. First, we aim to establish the feasibility of assessing the knowledge, attitudes and practices of current health behavior of older adults who have evidence of Type 2 diabetes, and how this differs by age, gender, HIV status and ART. We hypothesize that those co-infected with HIV and on ART will have greater awareness and knowledge of Type 2 diabetes due to increased contact with the health system. Second, we will evaluate strategies to assess the impact of Type 2 Diabetes and its common clinical sequelae such as diabetic retinopathy, peripheral neuropathy and diabetic neuropathy on functional status and productivity. We will explore how this may differ among those with HIV and on ART. The study will take place in 2017-18.
Evaluation of glycosylated haemoglobin for diagnosis of type 2 diabetes mellitus in Black African people with and without HIV (HbA1c) (sub- study of HAALSi/AWIGEN) Feb 2019
Project PI: Dr. Alisha Wade; Funder: South African National Research Foundation
Glycosylated haemoglobin (HbA1c) has been recommended by the World Health Organisation (WHO) as a method for diagnosing type 2 diabetes. There are, however, ethnic differences and differences between people with and without HIV that may make the WHO-specified thresholds for diagnosing diabetes inappropriate in Black Africans and people living with HIV. This study compares multiple methods of testing HbA1c with the gold standard oral glucose tolerance testing to evaluate whether WHO thresholds should be adjusted in these populations.
Endocrine and metabolic diseases in rural South Africa-establishing burden and improving detection Feb 2019
PI: Dr. Alisha Wade; Funder: Fogarty International Center, National Institutes of Health, USA
Endocrine and metabolic disorders (EMDs) are significant contributors to morbidity and mortality worldwide, but little is known about their relative prevalence in rural South Africa, where multiple independent risk factors such as HIV/AIDS, antiretroviral therapy, increasing life expectancy in adulthood and nutritional transitions interact in ways that likely make the relative burden of EMDs different from high income countries. Early detection and treatment of EMDs would reduce morbidity and mortality, but broad-based population screening in primary care is impractical in low resource settings. Integrating targeted case finding in those at highest risk for key EMDs into routine primary care may prove cost-effective. The long-term objective of this work to identify those individuals in South Africa at highest risk of key EMDs and their sequelae and to develop a cost-effective, pragmatic strategy for their long-term identification and management.
The African Research into Kidney Disease “ARK” Study
PI: Saraledevi Naiker; co-PI: June Fabian. Funders: SA-MRC, Newton Fund, GSK – as part of the Africa Open Lab initiative; and ISN (International Society of Nephrology)

This study seeks to determine the prevalence of chronic kidney disease, and explore associated clinical and genetic risk factors, in rural South Africa. Kidney disease forms part of an emerging non-communicable disease burden, which is poorly characterised in our country, and others from sub-Saharan Africa. The most common risk factors are hypertension, diabetes, obesity and HIV, which may occur concurrently. Other risk factors may be related to the use of traditional medicine, environmental toxin exposure and endemic infections such as bilharzia and malaria. Recently, genetic mutations have been identified that predispose African Americans to a more rapid progression of kidney disease and their origins have been traced to West African populations. These same mutations have been associated with severe kidney disease in HIV infected South Africans, but have not been explored in relation to other risk factors such as hypertension and diabetes. This study is part of a broader collaboration involving an urban site in Soweto, nested within the Birth to 20 cohort and sister rural and urban sites in Uganda and Malawi. Link to the ARK website here.
PROJECTS WITH COMPLETED FIELDWORK
Gender, pensions and social wellbeing in rural South Africa Nov 2017
Collaboration with INDEPTH, Colorado at Boulder and Missouri Univs, USA

Pension day, photo by L Hunter
This study is currently working on publications from primary and secondary dat to describe impact of old age pension on self-perceived health, well being and quality of life in older people and will explore gender differences and explain how policy changes in South Africa (reducing age eligibility of government pensions for men from 65 to 60 years) have influenced men’s perspective of health, wellbeing and quality of life. The latest paper from this work is titled “Living arrangements, disability and gender of older adults among rural South Africa“.
Activating Treatment as Prevention through Community Mobilization in South Africa Oct 2017
Increasing the number of South Africans who get tested and linked to care for HIV is important for many reasons. Researchers have found that HIV positive persons are much less likely to spread the virus to another person if they get on treatment early and stay on treatment. Using HIV treatment as a way of preventing HIV is called “Treatment as Prevention” (TasP). We believe that engaging communities in the process of “community mobilization” to learn as TasP is the best way to address barriers in order to improve testing, treatment and retention in care. Through a partnership between the MRC/Wits Rural Public Health and Health Transitions Research Unit, the Universities of California-San Francisco and North Carolina and two local organizations, Sonke Gender Justice and Right to Care, the community mobilization intervention (Tsima) will be implemented by Sonke Gender Justice from 2015 – 2018. At the end of the 3 years of intervention, we will look at the number of people who have been tested for HIV, are linked to HIV care, and remain in care in each village. To see if our intervention worked, we will compare these numbers between the 8 intervention villages and the 7 control villages to see if there is a difference.
To see a presentation with an overview of this study, click here. You can also read a peer reviewed paper titled ‘Evaluation of the Tsima CM intervention to improve engagement in HIV testing and care in South Africa: study protocol for a cluster randomized trial‘.
HIV patient outcomes after initiating HIV care and treatment in Agincourt, South Africa Oct 2017
Collaboration with Dr.Georges Reniers, London School of Hygiene and Tropical Medicine
Most HIV treatment programs in sub-Saharan Africa usually report about lost to follow-up (LTFU) – a composite unfavourable outcome – a general term for unknown outcomes of patients who have not returned for their next ART refill at a particular clinic. This variable amalgamates patients that have transferred their treatment to another clinic without proper documentation of the transfer, patients that have been misclassified either because of poor record keeping or human error, patients that have had a treatment interruption, patients that have stopped taking ART completely and patients that have died. This combination of outcomes underestimates retention and death rates by as much as five-fold while default rates are overestimated. With the expansion of treatment programmes in sub-Saharan Africa, more asymptomatic HIV patients initiating treatment, an important new population whose treatment behaviour might defer from that of earlier patients. Also, patients are now able to receive treatment in decentralized clinics much closer to their homes, potentially increasing loss to follow-up at pioneer HIV treatment clinics as patients move their treatment to more convenient locations. Using in-depth interviews, comprehensive record review at the clinics and review of tools for two non-profit organisations (Right-to-Care and Home Based Carers) tasked with tracing patients lost to follow-up, we will try to understand what loss to follow-up really means.
Health and wellbeing of ageing populations in Africa and Asia (SAGE) Feb 2019
Collaboration with INDEPTH sites, WHO, Umeå University, Sweden; University of Warwick, UK; Harvard, Washington, University of Colorado at Boulder, USA
In 2006 eight INDEPTH HDSS centres in Africa and Asia implemented a short version of the Study on Global Ageing and Adult Health (the SAGE study) instrument in coordination with WHO. Also in 2006-2007 the full version of the INDEPTH-WHO-SAGE Study was run in Vadu (India), Navrongo (Ghana) and Agincourt (South Africa) to allow for comparisons with the national WHO-SAGE study run in these countries (the SAGE national was also run in Russia, China and Mexico). The main objective of this study was to assess the health of the population 50 years and older by getting self-reported health and treatment coverage in different chronic conditions like hypertension, diabetes, stroke, depression…, and the evaluation of self-reported quality of life (WHOQoL) and functionality (WHODAS). The main findings were a high level of self-reported hypertension in both sexes, a higher level of self-reported lower health status and functionality in women, and an association of lower function and quality of life to higher mortality after following the Agincourt cohort for 3 years until 2009. Comparative and site-specific publications have been published. A part of this first round of data collection in Agincourt in 2006; there was a new round in 2010, including a module on health care utilization of people 50 years and older. Further analyses using the years of follow up in the HDSS sites and national comparisons using the 2006 data in the established cohorts is currently underway. An example of a published paper from this work is
The Nkateko Trial and Process Evaluation Feb 2019
Collaboration between the Division of Health Sciences, Warwick University UK, and the Centre for Health Policy and the Agincourt HDSS Unit, both part of the School of Public Health at Wits
Funded by the UK MRC, under the Global Alliance for Chronic Diseases programme.
The Nkateko cluster randomised trial built on earlier work in Agincourt which had shown a high and increasing prevalence of hypertension, poor management of hypertension, and problems for people in accessing care. The aim was to assess the effect of introducing lay health workers (LHW) into primary care clinics to assist the nurses, who provided the majority of the health care in such clinics. A recent government initiative to provide integrated chronic disease care had instituted major change in the clinics. There were many new tasks for the nurses, including setting up an appointments system, and pre-packing medication for patients. The hypothesis was that the LHWs would help with the new tasks, thus ensuring the system ran smoothly and releasing nurses to focus on providing good quality care. The outcome of the trial was measured by comparing the prevalence of poorly managed hypertension in before and after population surveys. An extensive process evaluation was put in place alongside the trial.
The trial is now complete. Read a summary of the results here. The results showed no effect on population prevalence of poorly managed hypertension, although patients in both intervention and control clinics showed an improvement in management. The process evaluation showed that intervention clinics had higher numbers of patients with hypertension attending regularly, and higher numbers coming on their appointed day. However, clinics were overwhelmed by rapidly increasing numbers of patients, partly due to the roll-out of anti-retrovirals and there were problems with the poor condition of the blood pressure machines and cuffs, drug outages for anti-hypertensives, an influx of inexperienced nurses and the challenging physical conditions of the clinic buildings. Because the care of patients with HIV is funded generously and vertically managed as a separate service, there was a tendency for management of hypertension to be regarded as a lesser priority.
The latest paper from Nkateko asks wether it is time to relook at policies for screening for hypertension – read the paper here.
HIV/NCD prevalence study (Ha Nakakela) Oct 2017
Collaboration with Wits Public Health, Colorado at Boulder and Washington Universities, USA
Study of 7,428 people aged 15 years and older to measure HIV prevalence, biomarkers for non-communicable chronic diseases (mainly cardiovascular and diabetes) using dried blood spots, physical measurements including blood pressure and anthropometry, and lifestyle and sexual risk behaviours. HIV result could be obtained at the health centre. Blood pressure and glucose results were given at the household with referral to nearest health facility for abnormal results.
HIV prevalence estimates by sex and age of residents in the MRC/Wits-Agincourt HDSS 2010

Papers emanating from this study include “Psychological and Socio-medical Aspects of AIDS/HIV” and
“Self-reported health and health care use in an ageing population in the Agincourt sub-district of rural South Africa”